
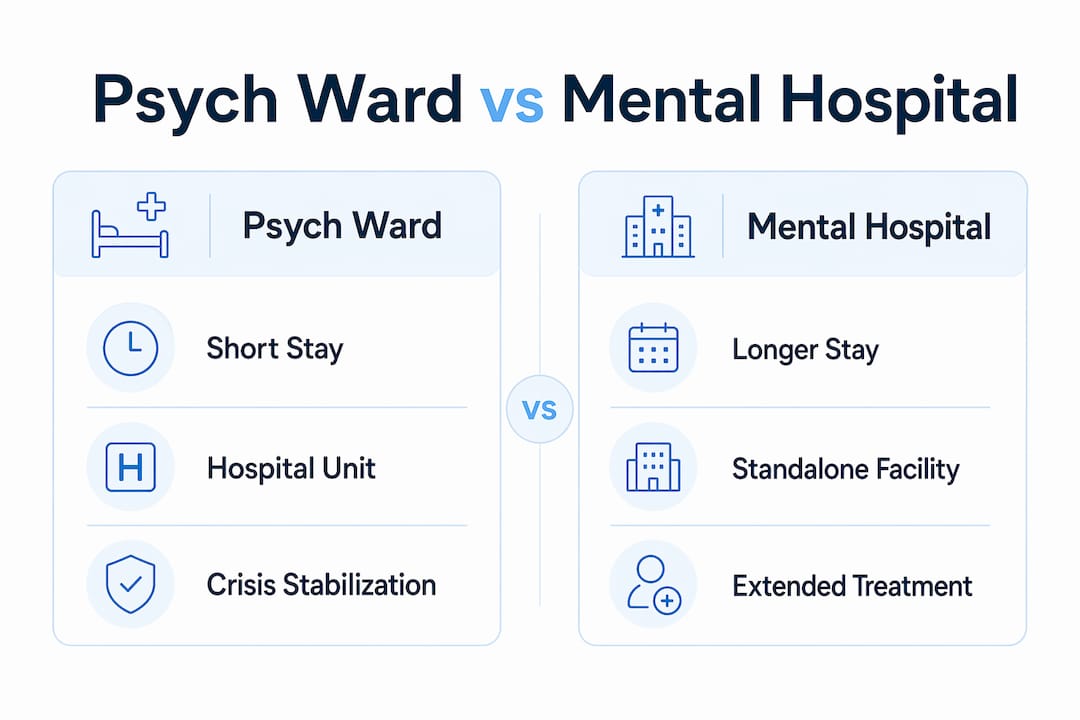
A psych ward is defined as a specialized psychiatric unit located inside a general hospital, focused on short-term crisis stabilization. A mental hospital, also called a psychiatric hospital, is a standalone facility dedicated entirely to mental health care, offering longer-term and more varied treatment programs. The core distinction is scope and setting: psych wards intervene during acute crises, while mental hospitals support recovery over weeks or months. For families in California navigating a mental health emergency, understanding this difference determines which level of care fits the situation and what to expect once a loved one is admitted.
What is a psych ward?
A psych ward is a locked, medically supervised unit inside a general hospital, designed to manage psychiatric emergencies. Patients arrive in acute distress, often following a suicide attempt, a psychotic break, or a severe mood episode. The unit’s primary goal is safety and stabilization, not long-term healing.
The average stay in a psych ward runs 7–10 days. That short window reflects the unit’s purpose: stop the immediate crisis, adjust medications, and arrange the next step in care. Deep therapy rarely happens during this period because the clinical team focuses on medical management and risk reduction first.
Admission to a psych ward follows two pathways:
-
Voluntary admission: The patient agrees to treatment and signs in willingly.
-
Involuntary hold: A clinician, law enforcement officer, or judge determines the patient poses a danger to themselves or others. California uses a 5150 hold under the Welfare and Institutions Code, which authorizes up to 72 hours of involuntary evaluation.
Psych ward features include strict safety protocols. Personal items such as shoelaces, belts, and certain electronics are restricted or confiscated on admission. Rooms are designed to minimize ligature points. Staff conduct regular checks, sometimes every 15 minutes. These measures exist to protect patients at their most vulnerable, not to punish them.
Treatment during a psych ward stay typically includes:
-
Psychiatric evaluation and diagnosis
-
Medication initiation or adjustment
-
Brief individual check-ins with a psychiatrist or social worker
-
Group psychoeducation sessions
-
Discharge planning that begins on day one
Pro Tip: If a loved one is admitted to a psych ward, ask the treatment team on the first day what the discharge criteria are. Knowing the clinical targets helps families prepare for the transition home.
A common misconception is that a psych ward stay resolves the underlying condition. Inpatient hospitalization is a temporary intervention aimed at stopping an acute crisis. Long-term healing happens in outpatient or residential settings after discharge.
What is a mental hospital?
A mental hospital, or psychiatric hospital, is a standalone facility built exclusively for mental health treatment. Unlike a psych ward embedded in a general hospital, a psychiatric hospital has no emergency room, no surgical suite, and no general medicine patients. Every resource on the campus serves psychiatric care.

Lengths of stay vary widely. Some patients spend two to four weeks in an acute inpatient program. Others stay months in a residential rehabilitation program. The facility’s structure allows for a pace of care that a psych ward cannot offer.
A psychiatric hospital typically provides a broader range of services:
-
Acute inpatient programs for patients who still need 24-hour supervision
-
Residential programs for patients who are stable but not yet ready for independent living
-
Partial hospitalization programs (PHP) that run five to six hours per day
-
Intensive outpatient programs (IOP) for step-down care
-
Specialized tracks for conditions like schizophrenia, bipolar disorder, or trauma
The environment inside a psychiatric hospital is meaningfully different from a psych ward. Psychiatric hospitals provide a quieter, more structured atmosphere that supports emotional regulation. Patients interact with the same peers and clinicians over days or weeks, which allows therapeutic relationships to develop. Group therapy, cognitive remediation, family psychoeducation, and vocational support all become possible when patients are stable enough to engage.
Pro Tip: When researching psychiatric hospitals in California, ask specifically whether the facility offers a step-down program. Moving from inpatient to a partial hospitalization program at the same facility reduces the risk of relapse during the transition.
Patient populations in psychiatric hospitals include people who have completed a psych ward stay and need continued structured support, as well as people who enter directly from the community when their condition requires more than outpatient care but less than emergency hospitalization.
How do treatment approaches and patient experiences differ?
The treatment goals in the two settings are fundamentally different. A psych ward targets immediate safety. A psychiatric hospital targets recovery and functional rebuilding.
| Feature | Psych ward | Psychiatric hospital |
|---|---|---|
| Setting | Unit inside a general hospital | Standalone dedicated facility |
| Average stay | 7–10 days | Weeks to months |
| Primary goal | Crisis stabilization | Rehabilitation and recovery |
| Therapy intensity | Minimal, psychoeducation focused | Group, individual, and specialized therapy |
| Environment | High turnover, clinical urgency | Quieter, structured, therapeutic |
| Admission type | Voluntary or involuntary hold | Primarily voluntary or step-down |
The day-to-day experience reflects these differences sharply. On a psych ward, patients may share space with others in acute distress. The pace is fast, staff rotations are frequent, and the clinical focus stays on medical stabilization. Patients often describe the environment as disorienting, particularly in the first 24–48 hours.
In a psychiatric hospital, the pace slows considerably. The quieter, supportive atmosphere allows patients to begin processing their experiences rather than simply surviving them. Structured daily schedules, group sessions, and consistent staff contact create a sense of predictability that supports emotional regulation.
Restraints and isolation are clinical safety tools used rarely and carefully in both settings. They are not punitive measures. Their use is documented, reviewed, and subject to strict regulatory oversight in California under the Department of Health Care Services.
Who needs a psych ward versus a mental hospital?
The decision between the two settings depends on clinical risk level and the patient’s current stability.
A psych ward is appropriate when:
-
The patient expresses active suicidal ideation with a plan or intent.
-
The patient poses an immediate danger to others.
-
A first psychotic episode requires urgent medical evaluation and medication initiation.
-
The patient cannot safely care for themselves due to severe psychiatric symptoms.
-
Medical complications accompany the psychiatric crisis, requiring general hospital resources.
A psychiatric hospital is appropriate when:
-
The acute crisis has resolved but the patient needs continued 24-hour supervision.
-
The patient requires intensive rehabilitation that outpatient care cannot provide.
-
Multiple prior hospitalizations suggest a need for longer-term structured treatment.
-
The patient’s condition, such as schizophrenia or schizoaffective disorder, requires a specialized program.
-
Family or social support at home is insufficient to maintain safety after discharge.
Voluntary and involuntary admission criteria apply to both settings, though involuntary holds are far more common in psych wards during acute crises. Clinicians use structured risk assessments to determine the appropriate level of care, weighing symptom severity, support systems, and treatment history.
What happens after discharge?
Discharge from either setting is not the end of treatment. It is the beginning of the most vulnerable phase of recovery.
Successful mental health outcomes depend on pre-arranged discharge plans that connect patients to outpatient care immediately after leaving the hospital. A gap of even a few days between discharge and the first outpatient appointment significantly increases relapse risk. This is especially true for patients with psychotic disorders, where medication continuity is critical.
Effective discharge planning includes:
-
A confirmed outpatient psychiatry appointment within seven days of discharge
-
A prescription for medications with enough supply to last until the first follow-up
-
Connection to a case manager or care coordinator
-
A crisis plan the patient and family understand and can use
-
Referral to a partial hospitalization or intensive outpatient program when appropriate
Pro Tip: Before a loved one is discharged from a psych ward or psychiatric hospital, confirm that the outpatient appointment is scheduled and that transportation is arranged. Do not assume the facility has handled these details.
California has invested in coordinated specialty care (CSC) models specifically to address the gap between inpatient discharge and stable community living. Programs built on the CSC framework, including Pandhealth’s approach in Los Angeles, combine psychiatry, therapy, family support, and vocational assistance into a single coordinated plan. This structure reduces the risk of rehospitalization and supports patients in rebuilding their lives after an inpatient stay.
Key Takeaways
A psych ward stabilizes acute psychiatric crises in days, while a mental hospital supports longer-term recovery through structured rehabilitation programs and coordinated specialty care.
| Point | Details |
|---|---|
| Setting and scope | Psych wards are hospital units; mental hospitals are standalone facilities with broader programs. |
| Length of stay | Psych ward stays average 7–10 days; psychiatric hospital stays range from weeks to months. |
| Treatment focus | Psych wards prioritize safety and medication; psychiatric hospitals prioritize recovery and skill building. |
| Admission criteria | Acute crisis and immediate danger drive psych ward admission; ongoing instability drives psychiatric hospital admission. |
| Discharge planning | Pre-arranged outpatient follow-up is the single most important factor in preventing relapse after discharge. |
What I’ve learned about inpatient care that most articles get wrong
Most writing about psych wards focuses on what they look like from the outside. Locked doors, restricted items, clinical staff. That framing misses the clinical logic entirely.
A psych ward is not designed to heal you. It is designed to keep you alive long enough to begin healing. That distinction matters enormously for families who expect a 10-day hospitalization to resolve a years-long condition. The ward does its job when a patient leaves stable enough to engage with real treatment. The real work starts after discharge.
What I find consistently underappreciated is the role of the discharge plan. Families focus on getting their loved one admitted. Clinicians focus on stabilization. Almost no one focuses enough on what happens on day 11. That gap is where relapse happens. The research is clear: advanced discharge planning is the single most protective factor in the transition from inpatient to community care.
The other thing worth saying plainly: safety measures in these settings exist because the patients inside them are in genuine danger. Restrictions on personal items, monitored environments, and clinical holds are not signs of a punitive system. They are signs of a system trying to protect people at their most vulnerable. Families who understand this tend to engage more constructively with the treatment team, and that engagement directly improves outcomes.
— eric
Pandhealth: specialized care when inpatient treatment ends
For many patients in Los Angeles, the hardest part of a psychiatric hospitalization is what comes next. Pandhealth was built specifically to address that gap.
Pandhealth provides coordinated specialty care for teens and young adults ages 13–35 experiencing thought disorders, including schizophrenia, schizoaffective disorder, and bipolar disorder with psychotic features. The program combines psychiatry, medication management, individual and group therapy, cognitive remediation, and family psychoeducation into a single coordinated plan. If you or someone you care about has recently been discharged from a psych ward or psychiatric hospital and needs structured outpatient support, contact Pandhealth to learn about next steps.
FAQ
What is the main difference between a psych ward and a mental hospital?
A psych ward is a unit inside a general hospital focused on short-term crisis stabilization, typically lasting 7–10 days. A mental hospital is a standalone facility that provides longer-term, more comprehensive psychiatric care including rehabilitation programs.
Can a patient be admitted to a psych ward against their will?
Yes. Patients can be admitted voluntarily or involuntarily based on risk assessment and legal criteria. In California, a 5150 hold allows up to 72 hours of involuntary psychiatric evaluation when a person is unable to provide food, clothing or shelter, or they pose a danger to themselves or others.
Is a psych ward the same as a mental asylum?
No. The term “asylum” refers to large, long-term custodial institutions that were largely closed in the United States during deinstitutionalization in the mid-20th century. Modern psych wards and psychiatric hospitals are medically supervised, rights-protected, and treatment-focused environments.
How long do patients typically stay in a psychiatric hospital?
Length of stay varies by program and patient need. Acute inpatient programs may last two to four weeks. Residential rehabilitation programs can extend to several months depending on clinical progress and treatment goals.
What should families do immediately after a loved one is discharged?
Confirm that an outpatient psychiatry appointment is scheduled within seven days of discharge and that medications are filled. Connect with a case manager or coordinated specialty care program to maintain continuity of treatment and reduce relapse risk.